Background
The term collision tumor is used when two unique neoplasms occur in the same organ at the same time. These tumors can be composed of 2 benign tumors, 2 malignant tumors, or a benign and a malignant tumor. Ovarian collision tumors are extremely rare with different combinations of the following tumors being cited in the literature: surface epithelial tumors, sex-cord stromal tumors, and germ cell tumors. While several cases of combined mucinous neoplasms and granulosa cell tumors have been identified, only one collision case of Sertoli Leydig Cell Tumor (SLCT) and high-grade serous carcinoma (HGSC) has been published (Kushida, Haba, Kadota, et al. 2005; McKenna, Kenny, Dorman, et al. 2005; Moid and Jones 2004; Smith and Paterson 2012; Subrahmanya, Kapadi, and Junaid 2011; Omo-Ogboi et al. 2022; Michalinos, Constantinidou, and Kontos 2015).
Methods
This case report, diagnosed in late 2022, includes the presentation, clinical management, and ultimately pathologic diagnosis of a rare collision tumor of the ovary composed on Sertoli-Leydig Cell Tumor and High-Grade Serous Carcinoma. A separate chart review was performed on this case including frozen and permanent section pathologic findings. Micropictographs were obtained from hematoxylin and eosin-stained slides.
Results
A 70 year old female, G4P4 with a medical history of hypothyroidism, intermittent palpitations, pre-diabetes, and prolonged QT interval presented to an outside emergency department for an episode of lightheadedness, dizziness, fatigue, and muscle weakness. Her blood pressure was elevated in the 200s and she was diagnosed with malignant hypertension. Her primary care provider worked her up for adrenal masses. A CT scan showed a potential right ovarian mass with omental caking, so she was referred to gynecologic oncology. At her referral, she reported feeling relatively well, except she had noticed becoming a little bit more unsteady, had a new mild tremor, increased facial fullness, and her daughter noted that her skin seemed darker than usual. The patient also noted that she had some abdominal bloating and felt a “twinge” on her right side occasionally. Additionally, she noted increased frequency of bowel movements and urination.
On physical exam her abdomen was soft, nondistended, no TTP throughout. A small umbilical hernia noted. Her CA-125 was 578 units/mL and testosterone 99.40 ng/dL. A CT was obtained showing extensive peritoneal carcinomatosis including omental caking, mesenteric nodules, and posterior pelvic peritoneal mass and a complex 5.0 cm solid cystic right ovarian lesion, suspicious for malignancy. Additionally small volume abdominopelvic free fluid was identified.
A transvaginal ultrasound was preformed highlighting an anteverted uterus with an endometrial thickness measuring 7.4mm. Her right adnexa contained a 3.64cm multicystic mass, possibly ovarian versus tortuous hydrosalpinx. The left ovary was not identified. The left adnexa contained a cystic tubular structure, likely hydrosalpinx. Again, trace amounts of free fluid were noted.
A PET scan was performed with the following impression: Diffuse FDG avid omental caking with numerous FDG avid peritoneal. Masses and nodules throughout the abdomen as well as numerous clustered FDG avid parauterine and left adnexal nodules. Findings were consistent with peritoneal carcinomatosis.

The patient was taken for diagnostic laparoscopy, right salpingo-oophorectomy, and biopsies of the omentum and pelvic peritoneum. In the OR, 1-4mm nodules scattered throughout the pelvic and abdominal peritoneum, small bowel mesentery, and diaphragm were noted. These nodules were nearly confluent on the falciform ligament and diaphragm. The right ovary was enlarged and cystic, with solid nodules on surface. The entirety of right fallopian tube was dilated and firm. The omentum adhered to anterior abdominal wall and falciform ligament while the posterior cul-de-sac was caked with firm tumor on peritoneum and anterior rectum. The bladder serosa was coated in firm tumor.

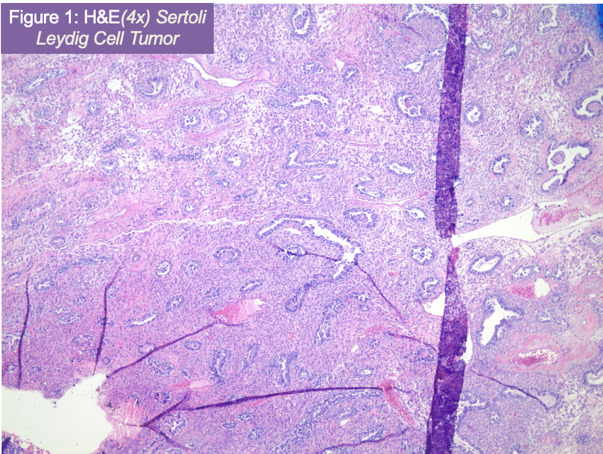
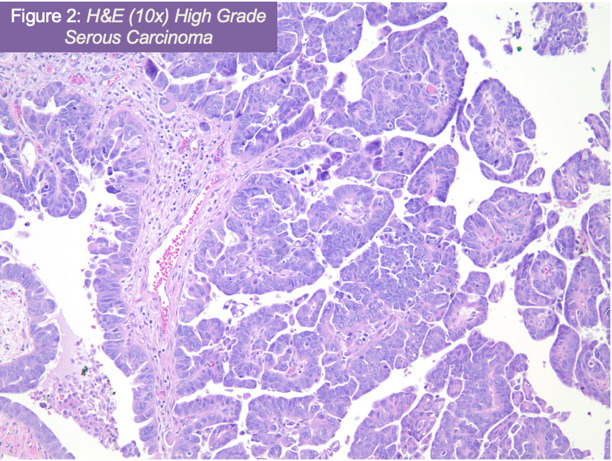
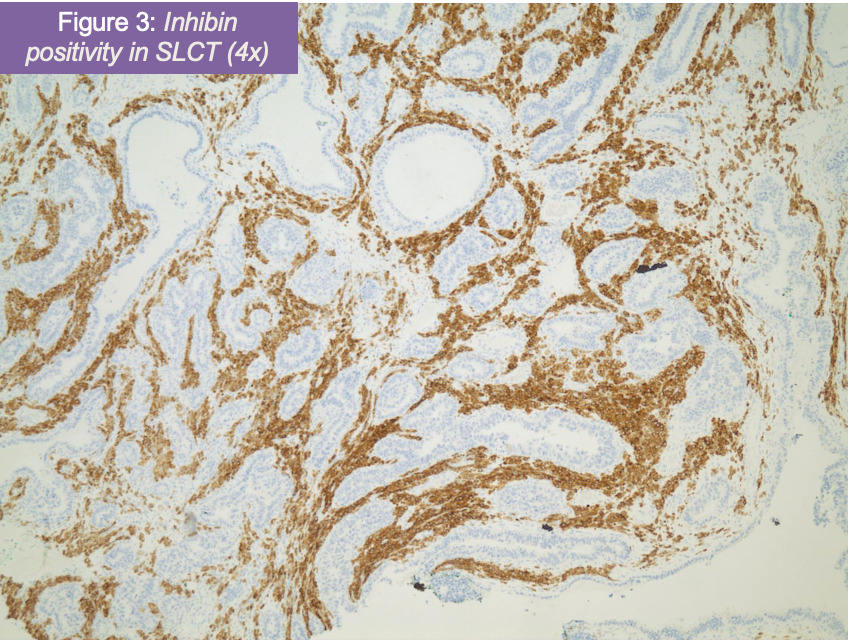
Pathologic review confirmed a poorly differentiated Sertoli-Leydig cell tumor (figure 1) of the right ovary (Stage IIIIC- pT3C Nx M0) with metastasis to the omentum and right pelvic side wall. Additionally, the right ovary was positive for high grade serous carcinoma (figure 2) metastatic from the fallopian tube. After H&E examination, immunostains for p53, napsin, PAX8, synaptophysin, CD56, and inhibin were ordered with adequate controls. Tumor cells corresponding to poorly differentiated Sertoli-Leydig tumor were positive for p53 (patchy), CD56, and inhibin (figure 3), while negative for PAX8, napsin, and synaptophysin. The metastatic high grade serous carcinoma was only positive for PAX8 and p53 (diffuse).

It was recommend to start IV Carboplatin/Taxol for 3 weeks for 6-8 cycles to cover both malignancies. Interval surgical debulking, either midway through chemotherapy or at completion of chemotherapy, depending on her response. A referral to cancer genetics for further genetic and molecular testing was provided. It was recommended for the patient to begin chemotherapy as the remainder of the disease was not resectable at the time and the possibility of interval debulking was discussed.
Discussion
Multiple theories have been suggested for how collision tumors develop, but the exact mechanism is unknown. The oldest and most straight forward theory is that each tumor developed independently of the other and by chance collided into each other (Omo-Ogboi et al. 2022). Another hypothesis suggests that these neoplasms originate from the same single cell that differentiates into two unique tumors, while another hypothesis suggests that one tumor can produce enough stromal changes to cause a second tumor to develop (Omo-Ogboi et al. 2022; “Collision Tumors: A Review of Their Types, Pathogenesis, and Diagnostic Challenges” 2020).
Serous carcinoma of the fallopian tube is the most common form of ovarian cancer, accounting for 70-80% of all ovarian carcinomas. They are classified as surface epithelial tumors and the average age range of diagnosis is 45 to 65 years. HGSCs are inherently high-grade, with morphologic features including significant cytologic atypia, high mitotic activity (threshold for HGSC defined as ≥ 12 mitotic figures per 10 HPF), and tumor giant cells. Architectural patterns may vary, including complex papillary, glandular, microcystic, and solid patterns. Ovarian HGSCs often express p53, p16, WT-1, and PAX-8 (Köbel, Kalloger, Huntsman, et al. 2010). Since they typically present at a stage III or IV, HGSCs are associated with a high mortality. The most common genetic mutations in HGSCs are in the p53 gene, which are present in up to 80% of tumors. Other common mutations are seen in NF1, BRCA1/2, RB1, and CDK12 (The Cancer Genome Atlas Research Network 2011).
It is now thought that most HGSCs originate from serous tubal intraepithelial carcinomas (STICs). STICs contain morphological changes consistent with precursor lesions such as increased proliferation, loss of polarity, nuclear atypia or enlargement, and atypical p53 expression. These precursor cells are believed to separate from the fallopian tube and travel to the peritoneum/ovaries, where they proliferate and become invasive. This hypothesis would account for why HGSCs often do not present until they have already progressed to a later stage (Visvanathan, Shaw, May, et al. 2018). Although HGSCs typically arise from the fallopian tube surface epithelium, they may also develop from the ovary or peritoneum epithelium (Kim, Park, Kim, et al. 2018).
Sertoli-Leydig cell tumors are a type of sex cord-stromal tumors (SCSTs). They are rare (5-10% of SCSTs) and typically found with Stage I disease. Stage III or IV are especially rare and there is little known on these neoplasms presenting at an advanced stage. Overall, data combining all stages of Sertoli Leydig tumors shows recommendation for chemotherapy and surgical resection. Prognosis of early-stage fallopian tube cancer is good while the prognosis of Sertoli Leydig cell tumor is more unknown. Most Sertoli Leydig tumors respond to chemotherapy, about half recur at 1-2 years based on limited data. The average age is 25 years with over 90% developing during the reproductive years. SLCTs typically produce sex-steroid hormones such as androgens, which can result in symptoms of androgen excess or virilization. However, 50% of patients display only nonspecific symptoms of an abdominal mass (Hoffman et al. 2020). The tumors can be solid or cystic grossly, but typically contain both solid and cystic components. SLCTs are classified as well-differentiated (tubular pattern), intermediately differentiated, or poorly differentiated (resembling the indifferent gonad). Most tumors are of intermediate differentiation and are not clinically malignant. About 22% of tumors were heterogenous and contained cell types foreign to the developing gonad, with the most common being mucinous gastrointestinal epithelium. Heterogenous elements such as skeletal muscle or cartilage can also be seen. A retiform pattern is observed in about 15% of tumors, which appears similar to the rete of the gonad and contains irregular, slit-like spaces with papillae (Young and Scully 1985). SLCTs have positive immunostaining for general sex cord proteins, including inhibin, calretinin, SF1, CD56, WT1, CD99, as well as vimentin and pancytokeratin from epithelial cells and MelanA/MART1 from Leydig cells (Soslow and Tornos 2011). Mutations in DICER1 and FOXL2 have been associated with SLCTs (Karnezis et al. 2019).
There have been other collision tumors reported with serous carcinomas. These include steroid cell tumor, granulosa cell tumor, and mature cystic teratomas (Bige, Demir, Koyuncuoglu, et al. 2009; Nirenberg, Östör, and Quinn 1992; Ozbey, Erdogan, Pestereli, et al. 2005; Singh and Singh 2014; Bichel 1985; Kajo and Macháleková 2007; Karki, Karki, Adhikari, et al. 2018). SLCTs have scarcely been observed in association with other tumors, but rare cases of collision tumors with serous cystadenomas and mature cystic teratomas have been observed (Stacher, Pristauz, Scholz, et al. 2010; Seo, Kwon, and Shim 1996; Bulwa and Lewis 1971; Seidman, Patterson, and Bitterman 1989).
Only one other case of a HGSC and SLCT collision tumor has been reported to our knowledge. Our case and the first case described both had tumors that were notably two separate entities with gross examination finding distinct masses. They were also both treated with Taxol and Carboplatin. However, there were a few small differences between these two cases. The case from our institution was composed of a SLCT primary to the ovary with the HGSC metastatic from the fallopian tube, whereas the first case described a HGSC primary in the ovary that metastasized to the fallopian tube. The SLCT at our institution was noted to be high grade, while the SLCT in the first case was intermittent grade. In addition, the patient in our case had high levels of CA-125, while the first case did not (Omo-Ogboi et al. 2022).
Conclusion
Sertoli-Leydig cell tumors are rare neoplasms seen even more rarely with a concurrent tumor in the ovary. Additionally, an advanced stage Sertoli-Leydig tumor makes this case even more unexpected. More research needs to be done to further understand collision tumors of the ovary and their associated findings and prognosis.